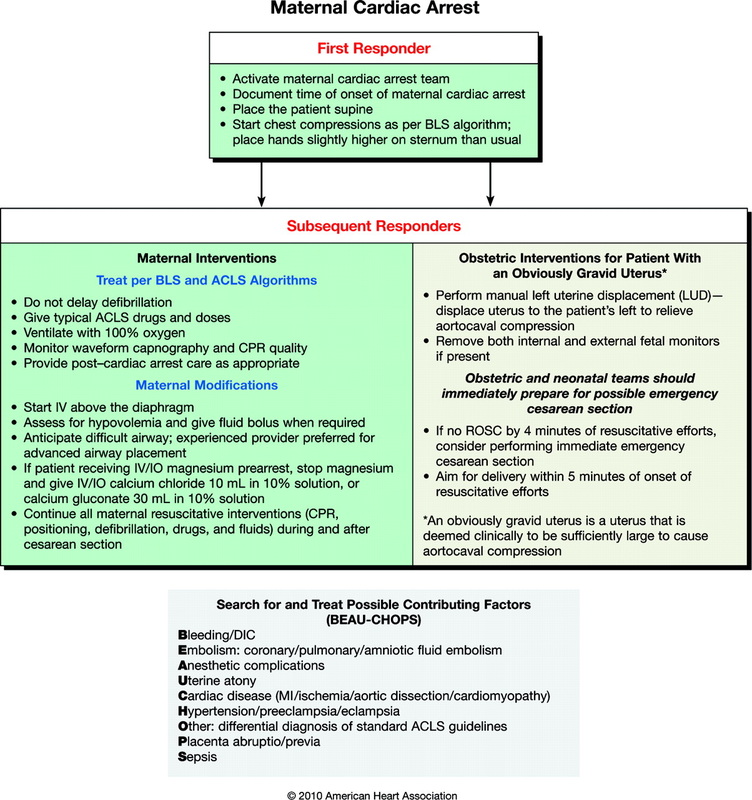
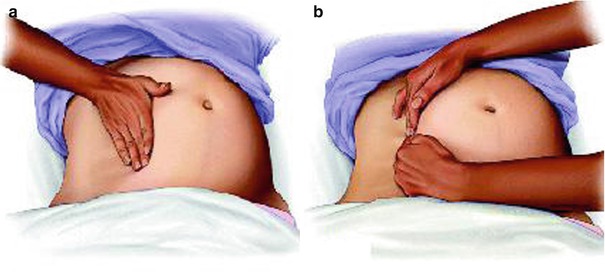
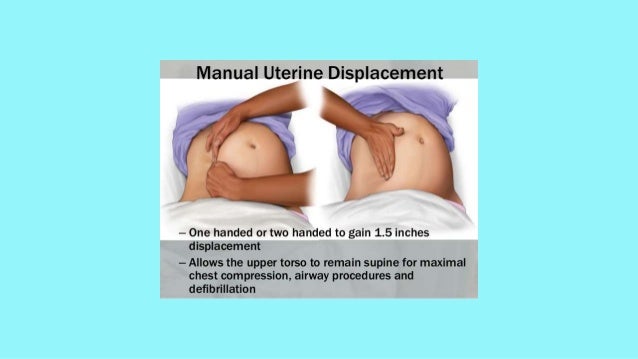
Manually Displace Uterus To The Left
O2 administration if needed in pregnant trauma patient.

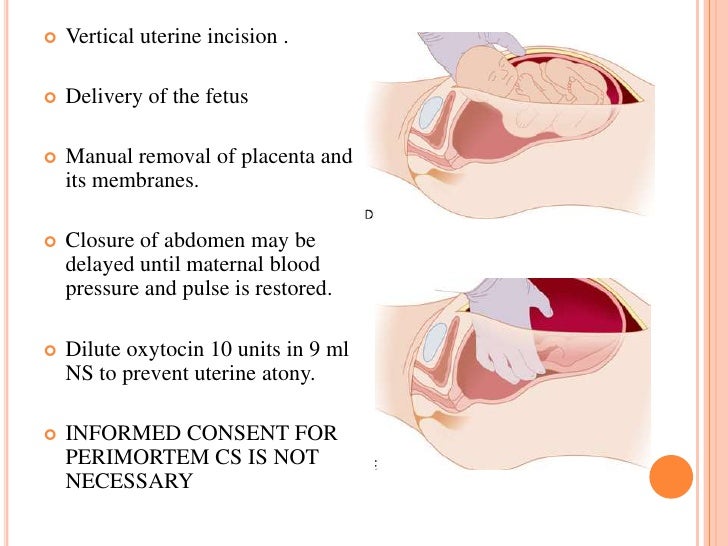
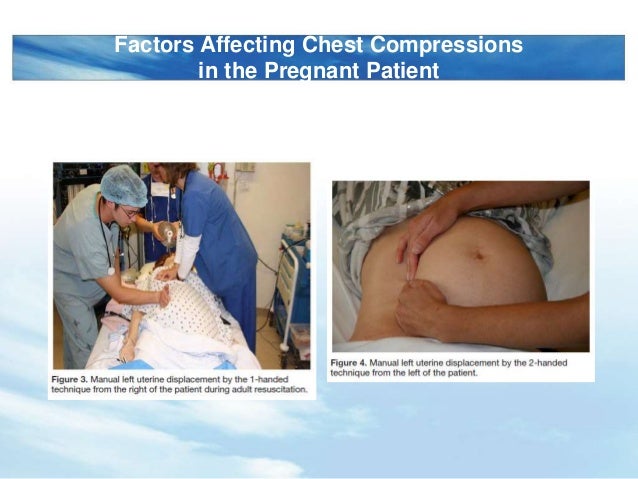
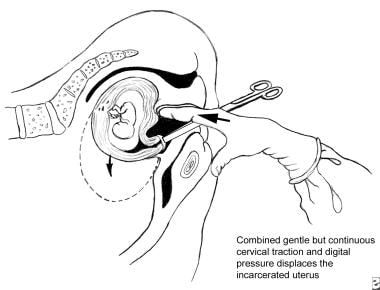
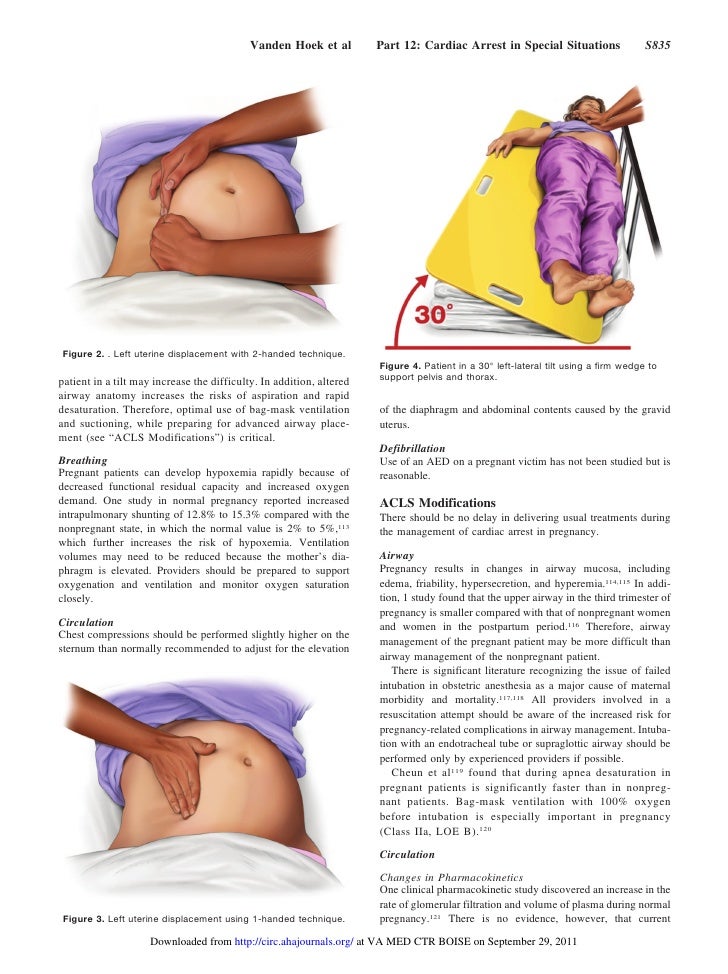
Manually displace uterus to the left. Gain intravenous access above the diaphragm. If the patient does not require spinal immobilization then she can be asked to assume the left lateral decubitus position. Many women are either born with a retroverted uterus or acquire one as they mature. Place four fingers through the opening in the broad ligament and grasp the entire broad ligament including the round ligament fig.
In most preparturient animals the broad ligament can be manually separated. The displacement of the uterus may be forward backward or lateral right or left. Falls and blunt trauma. With uterine anteflexion the angle between the body and cervix of the uterus is acute ordinarily it is no less than 900 and open to the front.
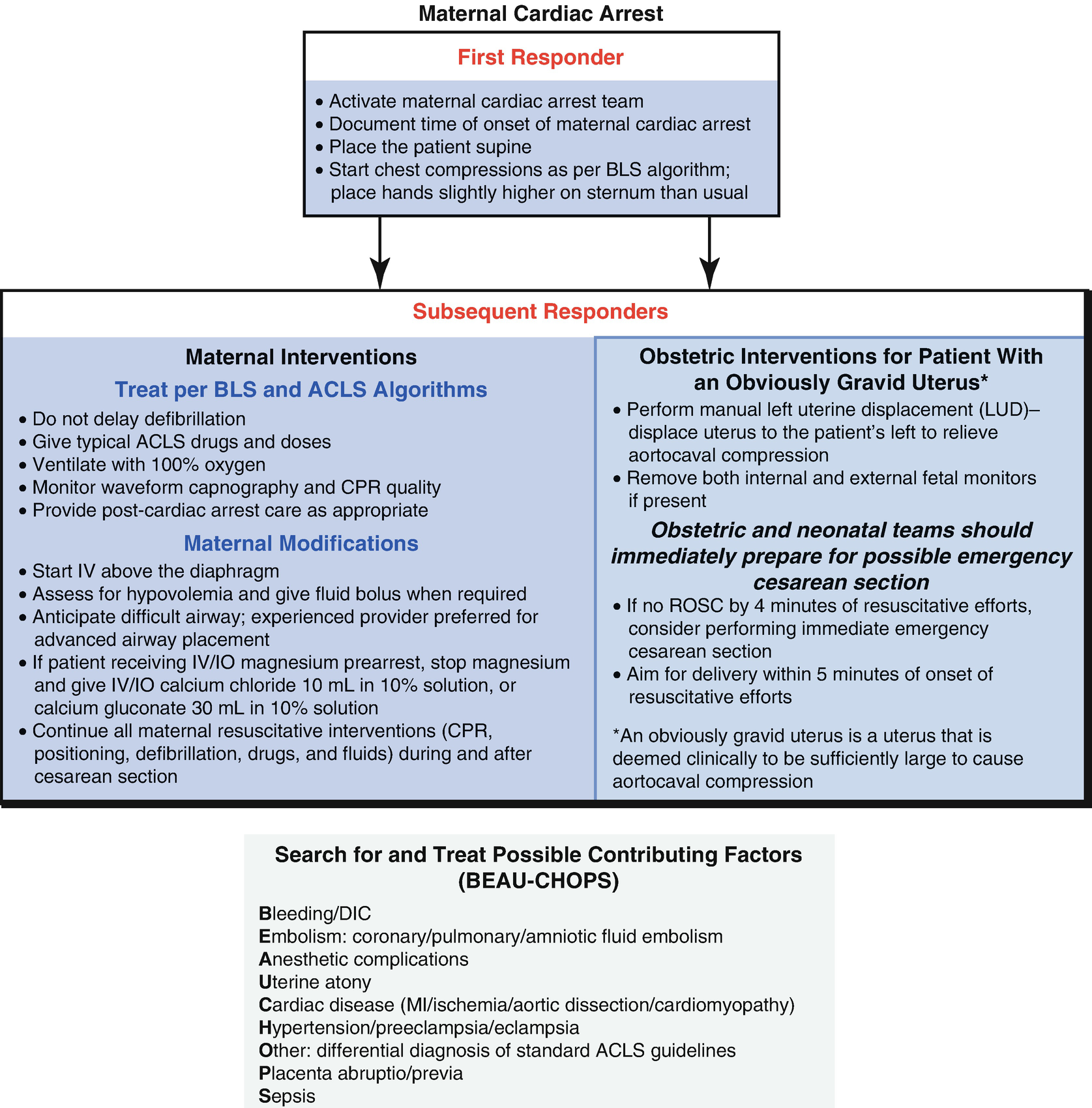
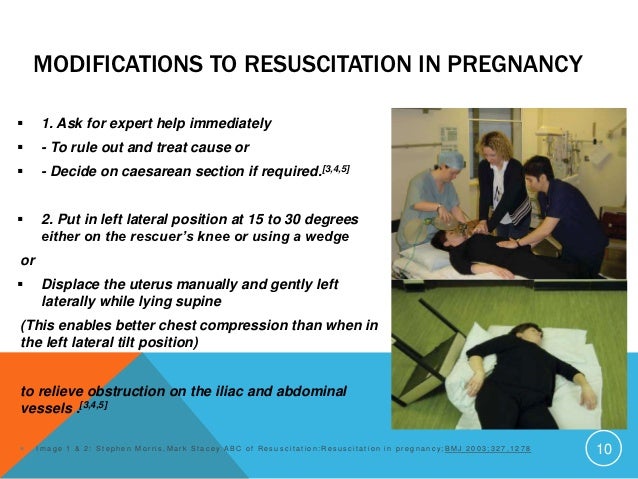
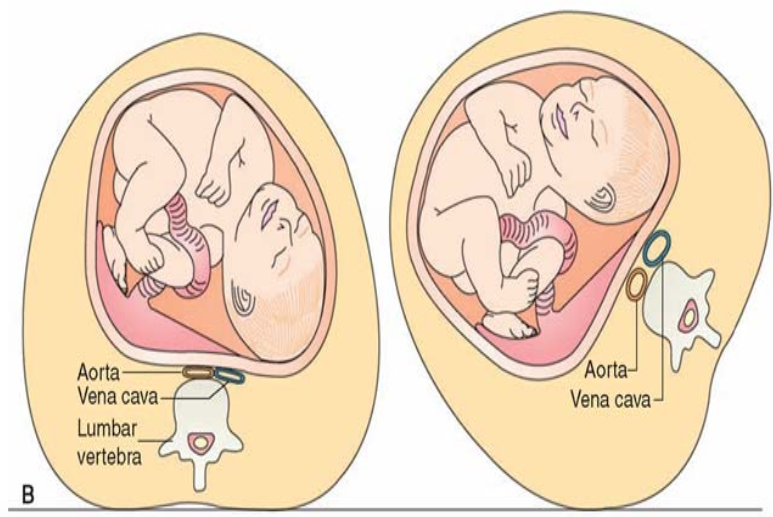
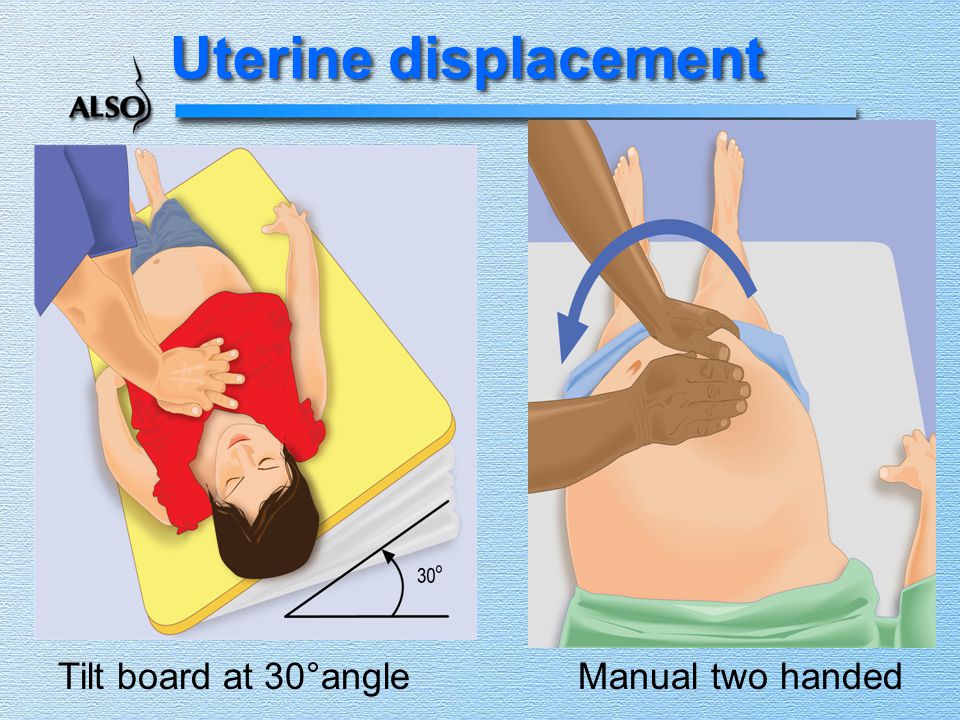
Manual leftward uterine displacement with resuscitation team 10. Most common complication of trauma in pregnant patient. Case series revealing that moving a woman from supine to a 45degrees left tilt or lateral position was an effective means of relieving the symptoms of aortocaval compression preceded the introduction of many different methods of uterine displacementthese included full lateral positioning. Alternatively one person may be designated to manually displace the uterus to the left.
A retroverted uterus is a uterus that curves in a backwards position at the cervix instead of a forward position. Placement of folded sheets waterbags airbags sandbags or rubber wedges under the hip or flank. Using backboard or hip wedge tilt patient 15 degrees to the left or right or manually displace uterus. Displace the gravid uterus off the great vessels either manually or with a left lateral tilt to avoid aortocaval compression.
Make an opening in the broad ligament adjacent to the uterine artery and vein close to the cervix fig. If the patient is more than 20 24 weeks pregnant the patient should be tilted 150 to the left. Ninety asa 1 and 2 pregnant women with term singleton pregnancies and no maternal and fetal complications scheduled for elective or emergency caesarean section were randomly allocated to group lt 150 left lateral table tilt n 45 and group md leftward manual displacement n 45subarachnoid block was established with a 25gauge spinal needle at the l3l4 interspace using 15 ml. Cause of most injuries in pregnancy.
Such displacement may be. Preoxygenate with 100 oxygen before intubation in anticipation of a more rapid onset of hypoxemia.

Remember That Young Healthy Women Can Lose A Lot Of Blood Before
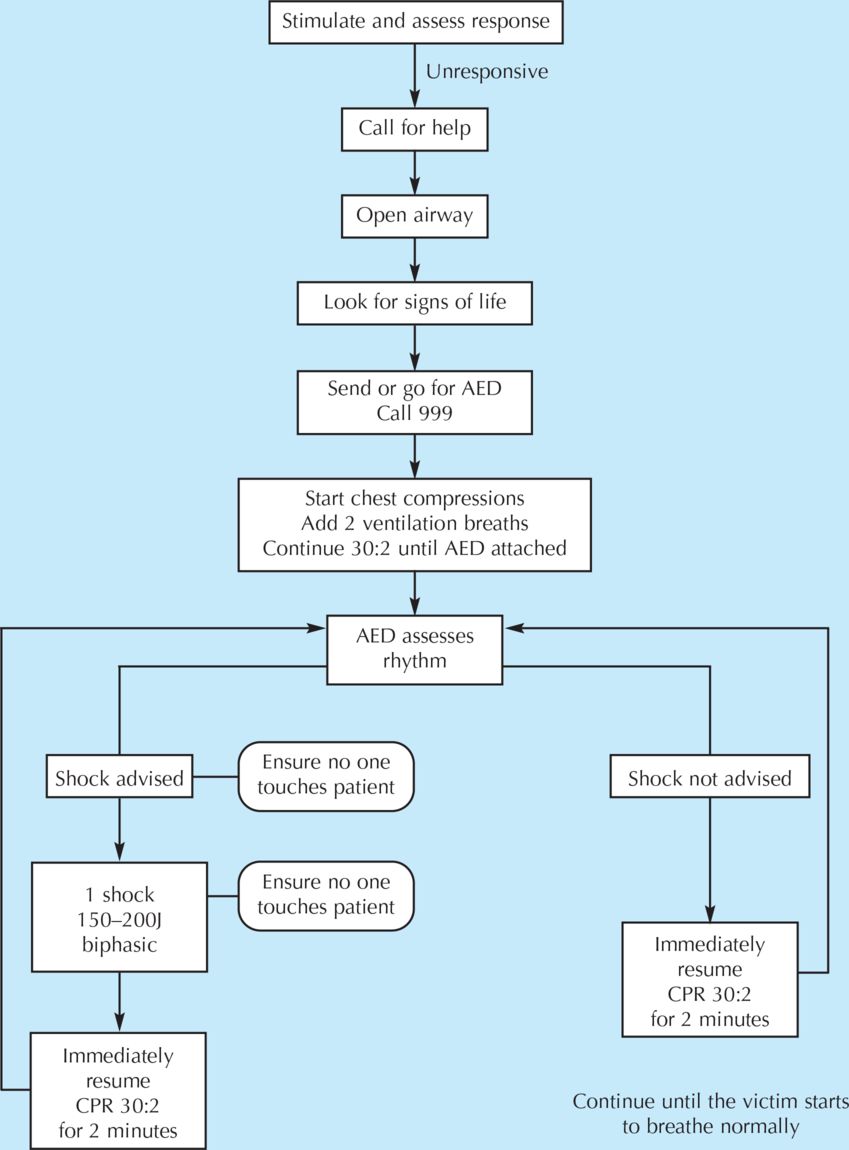
Cpr In Pregnancy Trauma In Pregnancy

Cardiac Arrest In Pregnancy Circulation

Trauma In Pregnancy Assessment Management And Prevention
Https Www Ahajournals Org Doi Pdf 10 1161 Cir 0000000000000300
































































Download Or Reading Online Manually Displace Uterus To The Left Here

